Seizures vs. Epilepsy: A Clear Comparison
Epilepsy creates unpredictable situations for people who have it, but researchers can quantify its impact on the entire nation. The 10-year projection from 2024 to 2033 shows that 82,723 new adult epilepsy patients will develop epilepsy. It predicts 15,227 deaths in this group and total healthcare costs of USD 14.2 billion.
It’s easy to underestimate epilepsy when you only see it case by case. These numbers show why epilepsy should be included in serious conversations about healthcare in Australia for 2026. In this blog, we explain the basics of epilepsy and connect the scale of its burden to timely diagnosis, access to treatment, and improvements in lifestyle or social support.
Key Takeaways
- The first signs of seizures that people experience during seizures differ significantly based on their age, the type of seizure, and which brain region is affected.
- A person who has one seizure episode does not automatically develop epilepsy because epilepsy requires more than one unprovoked seizure, which needs medical assessment to receive a proper diagnosis.
- Doctors diagnose seizures based on symptom observation and medical history, but they confirm seizure occurrence using video-EEG monitoring, which combines EEG results with video recordings.
- The first treatment for this condition should be medication, but patients with drug-resistant epilepsy need to receive vagus nerve stimulation as an additional therapy.
- Specialist consultation must occur for all seizure evaluations because new symptoms and injuries, pregnancy, and medication changes require urgent medical assessment.
Basic Understanding of Epilepsy and Seizures
What Is a Seizure?
A seizure is a brief episode in which the brain’s electrical activity becomes disorganized. What that looks like can vary a lot: some people have shaking and collapse, while others just stare, seem confused, make unusual movements, or “check out” for a few seconds and don’t respond as they typically do.
Common triggers: very low blood sugar, alcohol withdrawal, infections with fever, certain medications or drugs, sleep deprivation, or a head injury. Though sometimes we don’t find an apparent trigger right away. One important point: having a single seizure doesn’t always mean someone has epilepsy. Many people will have at least one seizure at some point in their lives.
What Is Epilepsy?
Epilepsy is a long-term brain condition where a person has a repeated tendency to have seizures that aren’t explained by a temporary, reversible trigger (like low blood sugar, alcohol withdrawal, or a high fever). It’s usually diagnosed based on a pattern over time, not on a single dramatic event.
About 51 million people worldwide live with epilepsy. Causes vary. Some cases relate to brain injury or scarring (including the hippocampus), while others are linked to genetic syndromes such as Juvenile Myoclonic Epilepsy.
Key Medical Meaning of Each Condition
Main Difference Between Epilepsy and Seizures
Is a Seizure Always Epilepsy?
Can a Person Have a Seizure Without Epilepsy?
How do Doctors Tell the Difference?
What Causes Seizures and Epilepsy?
Common Causes of Seizures
- Acute hits occur quickly and can catch you off guard.
- Low sodium disrupts neuron function, leading to serious issues.
- Alcohol withdrawal triggers storms in the frontal lobe, affecting behavior and cognition.
- Strokes in the temporal regions affect memory and language.
- Infections such as meningitis can cause brain swelling.
- Status epilepticus is a severe, ongoing condition that afflicts 9.9 to 41 per 100,000 annually.
- Some research links GLP-1 drugs like Ozempic to seizures in vulnerable people.
- Trauma causes about 20% of first-time adult seizures.
- Identifying and treating the trigger is crucial, as 70% of those affected never fully recover.
Common Causes of Epilepsy
- Structural causes
- Structural scars linger.
- Hippocampal sclerosis warps 15% of cases.
- Genetic causes
- Genetic glitches spark Dravet syndrome
- SCN1A mutations.
- Idiopathic
- Unexplained in about half of cases.
- Secondary epilepsy
- Secondary epilepsy climbed to 350 per 100,000 by 2021.
- Temporal malformations
- These affect adults specifically.
- Severe pediatric syndromes
- Lennox-Gastaut drops kids into multiple seizure hells.
Risk Factors for Each Condition
Genetics can play a role in epilepsy. Meaning, it may run in families, especially in types like juvenile myoclonic epilepsy (JME). Some seizures start after brain conditions such as a stroke.
In young children, seizures can sometimes happen with fever (febrile seizures). Birth complications like low oxygen (perinatal hypoxia) can also raise epilepsy risk later in life.
For people with epilepsy, frequent tonic-clonic (convulsive) seizures are linked to a higher risk of SUDEP (sudden unexpected death in epilepsy). Regular check-ups and reporting any seizure changes can help improve safety.
Types of Seizures and Epilepsy
Different Types of Seizures
- Severe pediatric syndromes
- Focal Aware - You’re awake and know what’s happening.
- Focal Impaired Awareness - You act a little confused. You might do small repetitive movements (e.g., fidgeting, chewing, etc.)
- Bilateral Tonic-Clonic - Starts in one spot but spreads.
- Generalized seizures (whole brain) – affect the whole brain from the start.
- Absence Seizures - You “zone out” or stare into space for a few seconds.
- Myoclonic Seizures - Involuntary brief jerks, of the arms or legs.
- Atonic Seizures - Muscles suddenly go limp.
Different Types of Epilepsy
- Focal Epilepsy – Seizures happen in one part of the brain.
- Generalized Epilepsy – Seizures start in the whole brain.
- Developmental/Genetic Epilepsy – Caused by genes, often harder to control.
How Types Affect Daily Life
- Tonic-clonic: driving/job restrictions.
- Atonic: fall precautions. Focal aware: often manageable.
- JME: Avoid sleep deprivation.
Symptoms to Watch For
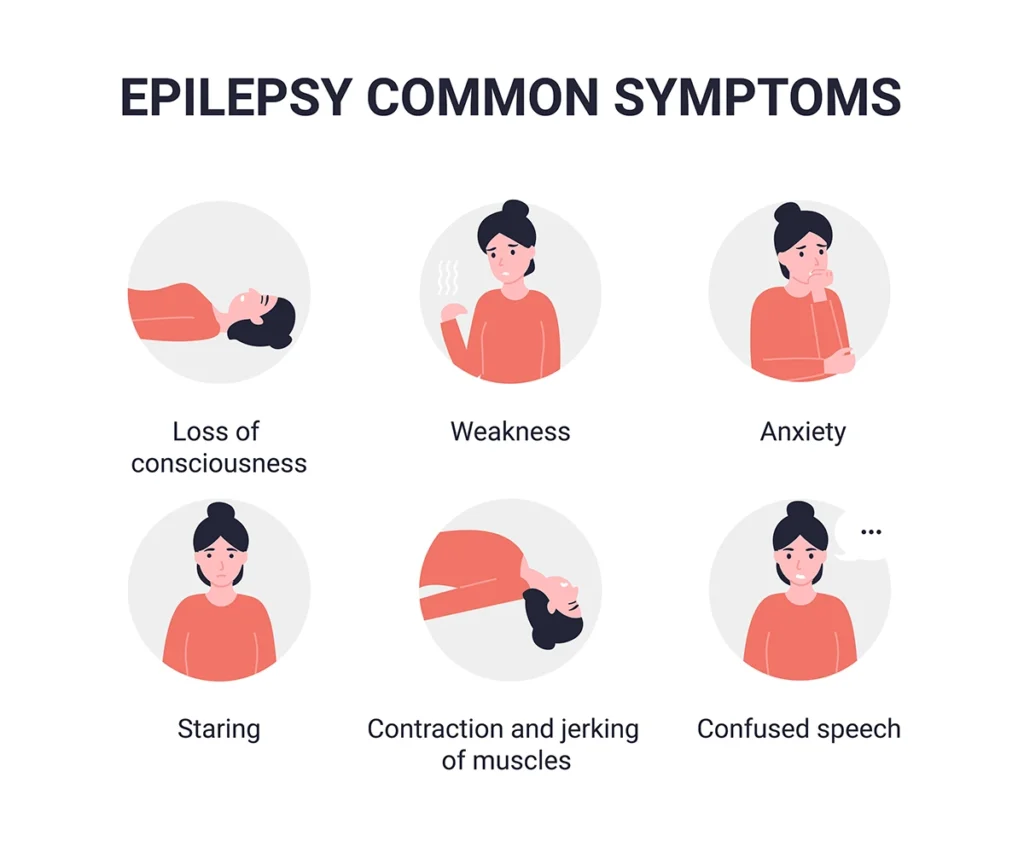
Symptoms of a Seizure
| Focal Seizures (one brain side) | Generalized Seizures (both sides) |
|---|---|
|
– Déjà vu or odd smells (temporal lobe) – Tingling, fear, lip-smacking – Staring, stiffening, falls |
– Tonic-clonic: complete shakes, blackout, bladder loss – Absence: 5-10 sec staring spells – Myoclonic: sudden jerks – Atonic: sudden drops |
Symptoms of Epilepsy
- Recurrent attacks + EEG spikes prove wiring issues
- Daily clues: chronic fatigue, memory gaps, mood swings
- Long-term: 50% cognitive fog, 30-50% depression/anxiety
- Temporal epilepsy bonus: emotional auras, hallucinations
Warning Signs Before a Seizure
- Irritability, insomnia, headache
- Nausea, déjà vu, odd tastes
- Pins-and-needles, rising panic
Your Condition May Qualify for Alternative Treatment
How Are They Diagnosed?
How Seizures Are Diagnosed
We start with your story; we ask what you felt before, during, and after the event. A witness description (and a phone video, if available) helps a lot, because timing and details matter.
Next, we look for reversible causes with blood tests (for example, glucose and sodium). We may do an EEG to check for abnormal brain electrical patterns, and a CT scan if there’s concern for head injury (MRI is often used later for a closer look). After a first seizure, we don’t always start daily medication right away. Your recurrence risk guides that decision, and we monitor it together.
Essential steps:
- Blood tests check metabolic causes (i.e., hyponatremia, glucose levels)
- Urgent EEG captures ictal rhythms in status epilepticus
- CT scan if trauma is suspected
How Epilepsy Is Diagnosed
Epilepsy is typically diagnosed after two unprovoked seizures, spaced 24 hours apart. A doctor may use an EEG (electroencephalogram) to look for abnormal brain activity, helping confirm a predisposition to seizures.
ILAE criteria at a glance:
| Must-Have | What It Shows |
|---|---|
|
Seizure history |
≥2 unprovoked events |
|
EEG |
Interictal spikes/discharges |
|
MRI |
Structural causes ruled out |
To capture real-world seizure activity, doctors sometimes recommend an ambulatory EEG,which monitors brain activity over a day or more in your usual environment.
ILAE criteria at a glance:
Medical Tests Used for Both
| Test | For Single Seizure | For Epilepsy |
|---|---|---|
|
EEG |
Catches active event
|
Shows spikes between |
|
MRI |
Spots an acute stroke |
Finds hippocampal sclerosis |
|
Video-EEG |
Confirms type |
ILAE 2025 classification |
|
PET/fMRI |
Metabolic check |
Surgery planning |
- The exact brain area responsible for seizures can be eliminated through surgical procedures, which achieve success rates of 60-80% for patients who have one specific seizure focus.
- The Vagus Nerve Stimulator (VNS) functions as a neck device that delivers soothing brain signals to reduce seizure frequency by 50%.
- The RNS brain implant system provides early seizure detection, enabling immediate brain stimulation to stop seizures.
- The laser ablation procedure uses laser technology to eliminate seizure sites through small surgical cuts.
By combining patient history, EEG results, imaging, and sometimes metabolic scans, doctors can form a clear picture of both the type of epilepsy and the safest, most effective treatment plan.
What Treatments Work?
Treatment for Seizures
Acute seizures demand immediate intervention while addressing the underlying trigger. Intravenous lorazepam (0.1 mg/kg) terminates status epilepticus within minutes, with intranasal midazolam serving as effective home rescue therapy.
Correct the cause:
- Hyponatremia: saline infusion
- Hypoglycemia: dextrose administration
- Alcohol withdrawal: supportive benzodiazepines
Treatment for Epilepsy
First-line anti-seizure medications achieve control in 60-70% when syndrome-matched:
- Keppra (20-60 mg/kg/day): minimal interactions
- Lamictal: mood stabilization bonus
- Depakote: JME gold standard
Lifestyle Changes That Help
Lifestyle changes won’t replace medicine, but they often make seizures less likely. Start with the basics: steady sleep, taking meds on time, limiting alcohol, managing stress, and writing down patterns or triggers. For some patients, especially certain childhood epilepsies, a ketogenic diet can help, but only with specialist supervision. CBT can be tremendous for stress and coping. And please teach the family simple seizure first aid. It really matters.
Living With Epilepsy vs Occasional Seizures
Daily Life with Epilepsy
Life After a Single Seizure
Safety Tips for Both Conditions
- Stay calm
- Make the environment safe (clear hazards)
- Side recovery position post-convulsion