Part 1: The 4 Types of Multiple Sclerosis Explained (Overview & Early Stages)
Introduction
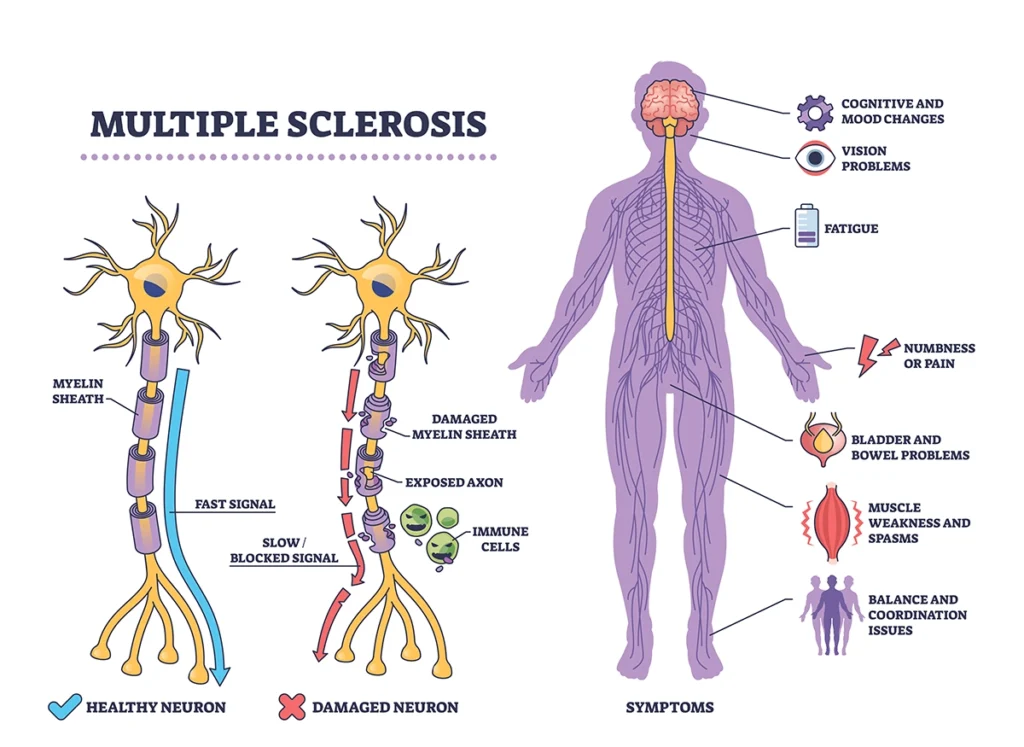
Multiple sclerosis (MS) is a condition in which the immune system mistakenly attacks myelin, the protective covering around nerve fibers in the brain, spinal cord, and optic nerves. Myelin helps messages travel quickly and smoothly between the brain and the rest of the body. When it becomes damaged, those messages can slow down or become disrupted.
Symptoms can vary from person to person but may include changes in vision, numbness or tingling, muscle weakness, problems with balance or coordination, bladder changes, fatigue, and difficulty with focus or memory. MS is most commonly diagnosed in young adults, though it can occur at any age.
The course of MS is not the same for everyone. Some people experience episodes of new or worsening symptoms followed by periods of recovery. Others may notice a gradual change in symptoms over time. A healthcare provider can help assess symptoms, provide a diagnosis, and discuss appropriate management options.
What Are the Types of Multiple Sclerosis?
Healthcare providers classify multiple sclerosis (MS) into four main patterns based on how symptoms develop and change over time:
- Clinically Isolated Syndrome (CIS): A first episode of neurological symptoms lasting at least 24 hours that is caused by inflammation or demyelination. CIS does not automatically mean a person has MS, but it may indicate a higher risk. Some individuals go on to develop MS, while others do not.
- Relapsing‑Remitting MS (RRMS): This is the most common form at diagnosis. It is characterized by clearly defined relapses, where new or worsening symptoms appear, followed by periods of partial or complete recovery (remission). Many people are initially diagnosed with this pattern.
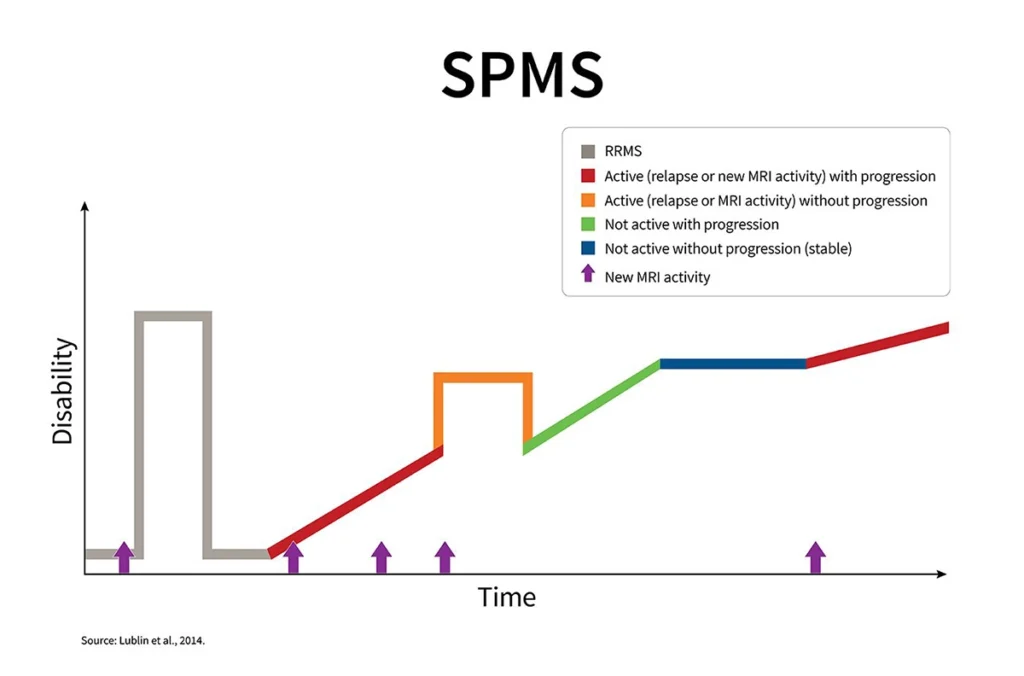
- Secondary Progressive MS (SPMS): Over time, some individuals with RRMS transition to a phase where symptoms gradually worsen between relapses. While relapses may still occur, the primary feature becomes a steady progression of disability.
- Primary Progressive MS (PPMS): In this form, symptoms gradually worsen from the onset without distinct relapses or remissions.
Updated terminology:
The term “progressive-relapsing MS” (PRMS) was used in the past. Current guidelines no longer use this label. Instead, clinicians describe progressive MS as either “active” (if there are relapses or new MRI activity) or “not active,” which helps guide treatment and monitoring decisions.
Why Multiple Sclerosis Is Classified Into Types
The four types of multiple sclerosis are not personal identifiers. They are clinical classifications that describe how the condition is behaving over time. Understanding the pattern of disease activity helps the care team choose the most appropriate approach and monitor changes more effectively.
Classification serves several important purposes:
- Improves communication: It provides a shared clinical framework for patients, healthcare providers, and researchers.
- Sets expectations: While it cannot predict the future with certainty, it helps outline how the condition may evolve over time.
- Guides treatment decisions: Certain therapies are more effective for relapsing forms of MS, while others are used when there is gradual progression.
- Supports research and insurance processes: Clinical trials and coverage decisions are often based on MS classification and whether the disease is currently active.
Current terminology also includes additional descriptors such as “active” or “not active,” as well as whether there is evidence of progression. These distinctions provide a more detailed understanding beyond the primary classification.
How MS Types Affect Symptoms and Progression?
Many symptoms can occur across all four forms of multiple sclerosis. What distinguishes each type is not the specific symptoms themselves, but the pattern in which they develop over time. Some forms are characterized by clearly defined relapses followed by recovery, while others involve a gradual worsening of symptoms. Recognizing this pattern is important because it guides treatment decisions and helps the care team monitor changes through clinical exams and MRI findings.
- CIS: involves a single episode of neurological symptoms. The specific symptoms depend on the area of the central nervous system affected, such as the optic nerve, spinal cord, or brainstem. Ongoing evaluation, including MRI imaging, helps determine the likelihood of developing MS.
- RRMS: is marked by episodes of new or worsening symptoms (relapses), followed by periods of partial or complete recovery (remissions). Recovery can vary from person to person. Over time, some residual symptoms may remain after relapses.
- SPMS: typically begins as RRMS and later transitions into a phase of gradual symptom progression. While relapses may still occur, steady worsening becomes more prominent.
- PPMS: involves a gradual progression of symptoms from the onset, without clearly defined relapses or remissions.
Regular follow-up appointments and MRI monitoring are essential in all forms of MS. These assessments help track disease activity, evaluate progression, and inform treatment planning.
Relapsing-Remitting Multiple Sclerosis (RRMS)
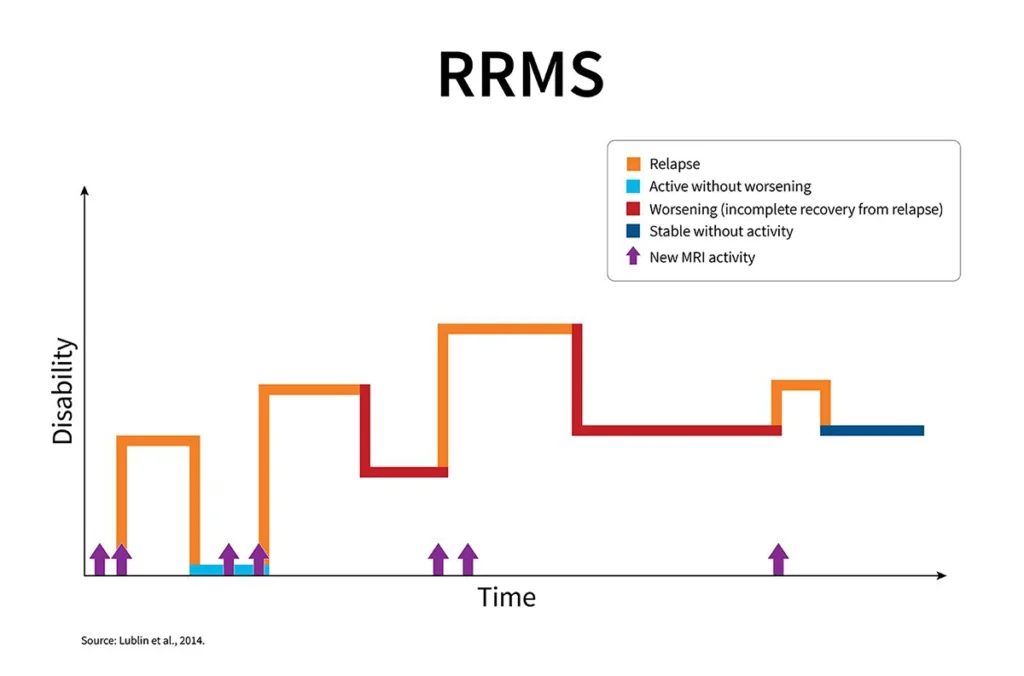
RRMS is the most common form of MS at the time of diagnosis. Approximately 85 percent of individuals with MS are initially diagnosed with this pattern. RRMS is characterized by clearly defined episodes of new or worsening symptoms, followed by periods of recovery.
During recovery phases, also known as remissions, symptoms may partially or completely improve. In some cases, certain symptoms may persist. Over time, some individuals with RRMS may transition to a more steadily progressive form of MS known as secondary progressive MS (SPMS). However, RRMS is the most common starting point.
What Is Relapsing-Remitting MS?
RRMS follows a pattern of relapses and remissions.
A relapse occurs when new neurological symptoms develop or existing symptoms worsen, typically lasting at least 24 hours and not explained by another cause such as infection.
A remission refers to a period of symptom improvement or stability following a relapse. Recovery may be substantial, and in some cases complete.
Identifying this pattern is important because treatment strategies for RRMS focus on reducing the frequency of relapses, limiting new MRI activity, and slowing long-term disease progression. Regular monitoring helps guide these decisions and assess how well treatment is working.
Common Symptoms of RRMS
Symptoms of RRMS vary from person to person. The specific symptoms experienced during a relapse depend on the area of the central nervous system affected by inflammation. Because different parts of the brain and spinal cord control different functions, symptom patterns can differ significantly between individuals.
Symptoms of RRMS vary from person to person. The specific symptoms experienced during a relapse depend on the area of the central nervous system affected by inflammation. Because different parts of the brain and spinal cord control different functions, symptom patterns can differ significantly between individuals.
- Common symptoms during a relapse
During a relapse, individuals may experience one or more of the following:- Numbness or tingling in the face, arms, legs, or torso
- Significant fatigue that goes beyond typical tiredness
- Muscle weakness, stiffness, or spasms
- Difficulty with balance, coordination, or walking
- Vision changes, such as blurred or double vision, partial vision loss, or eye discomfort
- Sensitivity to heat, which may temporarily worsen symptoms
- Bladder or bowel changes, including urgency, frequency, or constipation
- Dizziness or lightheadedness
- Cognitive changes, often described as “brain fog” or slowed thinking
- Changes in mood, including low mood or anxiety
Some individuals may also experience nerve-related pain, burning sensations, or an electric-shock sensation down the back when bending the neck (known as Lhermitte’s sign).
- How symptom location influences experience
Symptoms often reflect the area of inflammation:
- Optic nerve involvement: Eye pain with movement, blurred or dim vision, reduced color clarity
- Spinal cord involvement: Leg weakness or stiffness, numbness below a certain level, bladder urgency
- Brainstem or cerebellum involvement: Double vision, vertigo, coordination or balance difficulties
- Areas involved in thinking and processing: Slowed information processing, difficulty finding words, or concentration challenges
- Symptom patterns
- Fatigue is one of the most commonly reported symptoms.
- Walking or balance difficulties may develop.
- Numbness or tingling can occur in different areas of the body.
- Vision changes may be present.
- Bladder urgency or frequency can occur.
- Cognitive changes, such as slowed thinking or difficulty concentrating, are also common.
- Symptoms may appear together and can affect mobility, energy levels, mood, comfort, and daily functioning.
- Heat sensitivity and temporary symptom worsening
- Heat exposure, fever, or infection can temporarily worsen existing symptoms.
- This is often referred to as a pseudo-relapse.
- Symptoms may feel more intense but do not indicate new inflammatory damage.
- Cooling down and addressing triggers such as infection typically leads to improvement.
- Typical course of a relapse
- Relapses often develop gradually over several days.
- Symptoms may improve over weeks to months.
- Recovery can be partial or complete.
- Some individuals may experience lingering symptoms after a relapse.
- Early recognition and appropriate treatment can help reduce long-term impact.
- The importance of symptom tracking
- Keeping a simple record of symptoms can support care decisions.
- Note when symptoms began and how severe they became.
- Record possible triggers, such as heat or infection.
- Track how much recovery occurred and how long it took.
- Report new neurological symptoms lasting more than 24 hours without a clear trigger to a healthcare provider.
- The degree of recovery during remission can provide valuable insight for long-term care planning.
Secondary Progressive Multiple Sclerosis (SPMS)
SPMS develops in some individuals who were previously diagnosed with relapsing-remitting MS (RRMS). It is not a separate condition, but rather a change in the pattern of disease activity over time.
In RRMS, symptoms typically follow a pattern of relapses and remissions. In SPMS, the pattern shifts toward a more gradual and steady progression of symptoms.
What changes?
- The primary change is in the pattern of progression, not necessarily the types of symptoms experienced.
- Instead of clear periods of relapse and recovery, there is a gradual worsening of function over time.
- Relapses and new MRI activity can still occur. When this happens, it is referred to as active SPMS.
- SPMS can also be described as not active when there are no recent relapses or new MRI findings.
- Progression (gradual worsening) is assessed separately from activity, meaning progression can occur even without new MRI lesions.
How the pattern evolves
- In RRMS, disability often increases in noticeable steps associated with relapses.
- In SPMS, disability tends to increase more steadily over months or years.
- Changes may be subtle at first, with gradual shifts in strength, mobility, or endurance.
- Determining SPMS is based on observing long-term patterns, not on a single difficult week.
What this means for care:
- Treatment goals may shift toward slowing long-term progression and preserving function.
- Decisions about therapy consider whether the disease is active or not active.
- Rehabilitation, mobility support, and symptom management often play a larger role in care planning.
- Ongoing monitoring remains important to guide treatment adjustments.
SPMS represents a change in how MS behaves over time. Understanding this pattern helps healthcare providers tailor care strategies to support long-term function and quality of life.
How RRMS Can Progress Into SPMS?
The transition from RRMS to SPMS typically occurs gradually rather than suddenly. Instead of disability increasing only during relapses, there is a steady progression of symptoms between episodes over time.
What research shows
- Earlier long-term studies suggested that approximately 10 percent of individuals transitioned to SPMS within 10 years of diagnosis, about 50 percent by 20 years, and a majority by 30 years.
- More recent registry data indicate that modern disease-modifying therapies may delay this transition and reduce the overall number of individuals who progress to SPMS.
- Healthcare providers base the diagnosis of SPMS on sustained, objectively documented worsening over 6 to 12 months following a relapsing phase, rather than on a single relapse or temporary decline.
Signs of possible transition
- Shorter periods of stability between symptom flare-ups
- Subtle but steady worsening in mobility, balance, or endurance
- Increased difficulty with walking
- Changes in bladder function
- Cognitive changes
- Persistent fatigue that gradually worsens over time
These changes are typically observed over months, not days or weeks.
Factors associated with earlier progression
- Older age at MS onset
- Greater disability early in the disease course
- A higher number of relapses in the initial years
Why monitoring matters
Regular follow-up helps determine whether MS remains in a relapsing pattern or is showing signs of progression. Clinicians may describe the disease as “active” (with relapses or new MRI activity) or “not active.” This distinction helps guide treatment decisions and long-term care planning.
Symptoms Common in SPMS
Many of the symptoms seen in SPMS are similar to those experienced in RRMS. The key difference is that in SPMS, symptoms tend to be more persistent and gradually progressive rather than occurring mainly during relapses.
Common symptoms may include:
- Increasing difficulty with walking or balance, including feeling unsteady or slower on your feet
- Muscle weakness, stiffness, or spasticity, particularly in the legs
- Sensory changes such as numbness, tingling, burning, itching, or nerve-related pain
- Ongoing fatigue that persists beyond occasional tiredness
- Bladder or bowel changes, including urgency, frequency, or constipation
- Vision changes, such as blurred or double vision, or partial vision loss
- Cognitive changes, including slowed thinking, memory concerns, or difficulty finding words
- Dizziness or vertigo
- Changes in mood, including anxiety or low mood
If you notice gradual, steady changes in your baseline function, even without clear relapses, it is important to discuss this with your healthcare provider. Identifying patterns of progression early can help guide treatment decisions and supportive care strategies.
Understanding the early and intermediate patterns of multiple sclerosis is an important first step. In Part 2, we’ll explore progressive forms of MS in more detail, how diagnosis is made, how disease patterns can change over time, and what management and treatment approaches may look like across different types.