Part Two: Progressive MS, Diagnosis, and Management
Introduction
While relapsing and secondary progressive forms of MS are more commonly discussed, other patterns of disease progression are equally important to understand. This section focuses on primary progressive MS, historical classifications, how MS is diagnosed, and how care is tailored over time.
Primary Progressive Multiple Sclerosis (PPMS)
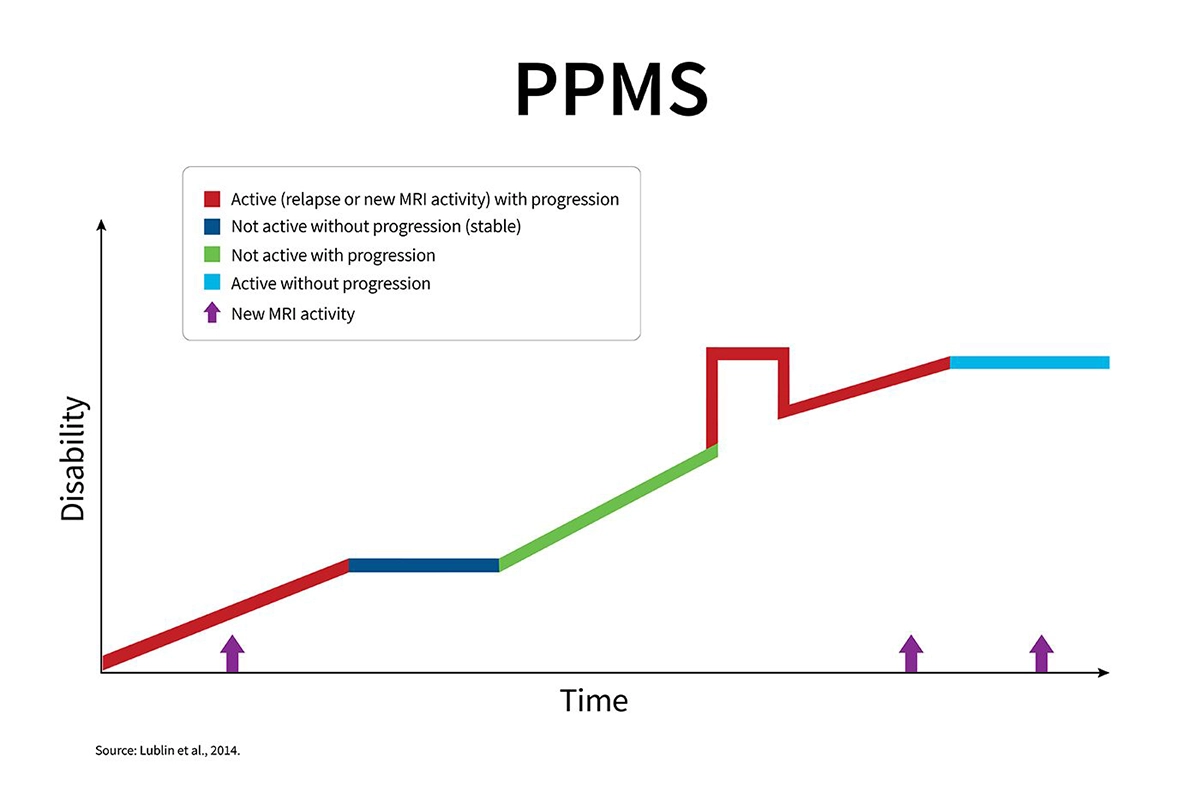
Primary progressive multiple sclerosis (PPMS) is characterized by a gradual and continuous progression of symptoms from the onset of the condition. Unlike relapsing forms of MS, PPMS does not typically involve clearly defined relapses followed by periods of recovery. Instead, symptoms slowly build over time.
PPMS is less common than relapsing forms of MS, affecting approximately 10 to 15 % of individuals diagnosed with multiple sclerosis. It also tends to be diagnosed at a slightly older average age compared to relapsing-remitting MS.
While the progression is generally steady, the rate of change can vary from person to person. Ongoing monitoring and individualized care planning remain essential to managing symptoms and maintaining function.
What Makes PPMS Different?
Primary progressive multiple sclerosis (PPMS) is defined by gradual progression of disability from the onset of symptoms. Unlike relapsing forms of MS, there are no early periods of clear relapses followed by recovery. Instead, clinicians diagnose PPMS when there is sustained, objectively documented worsening over time, often observed over a period of 12 months or more.
Key characteristics of PPMS include:
- Progression from the beginning: Symptoms gradually worsen from onset without the classic relapse-and-remission pattern.
- Less inflammatory activity on MRI: Compared with relapsing MS, there are often fewer contrast-enhancing lesions, reflecting a more gradual disease process.
- Spinal cord involvement: PPMS more commonly affects the spinal cord, which is why walking and balance difficulties are often early symptoms.
- Lower overall frequency: PPMS accounts for approximately 10 to 15 % of MS cases.
- Later onset: It is often diagnosed at a slightly older age compared with relapsing forms of MS, with a somewhat higher proportion of men affected.
Although PPMS and secondary progressive MS (SPMS) may appear similar once steady progression is established, the distinction lies in how the disease begins. PPMS is progressive from the outset, whereas SPMS develops after an initial relapsing-remitting phase.
Early Signs of Primary Progressive MS
Early PPMS symptoms often develop gradually rather than appearing as sudden flare-ups. Instead of distinct attacks, individuals may notice subtle changes that slowly progress over time.
Common early signs may include:
- Increasing difficulty with walking, such as slower pace, subtle changes in gait, tripping more frequently, or legs feeling weak or stiff (spasticity)
- Reduced balance, making stairs or longer distances more challenging
- Persistent fatigue that does not resolve with rest
- Sensory changes, including numbness, tingling, pins-and-needles sensations, burning, or nerve-related pain, often affecting the legs, feet, or back
- Bladder or bowel changes, such as urgency, frequency, or constipation
- Vision changes, including blurred or double vision
- Dizziness or vertigo
- Cognitive changes, such as slowed thinking or difficulty concentrating
- Changes in mood, including low mood or increased anxiety
If you notice gradual and steady changes rather than clearly defined relapses, it is important to discuss these symptoms with your neurologist. Keeping a record of changes over weeks or months can help identify patterns and support timely evaluation and care planning.
Progressive-Relapsing Multiple Sclerosis (PRMS)
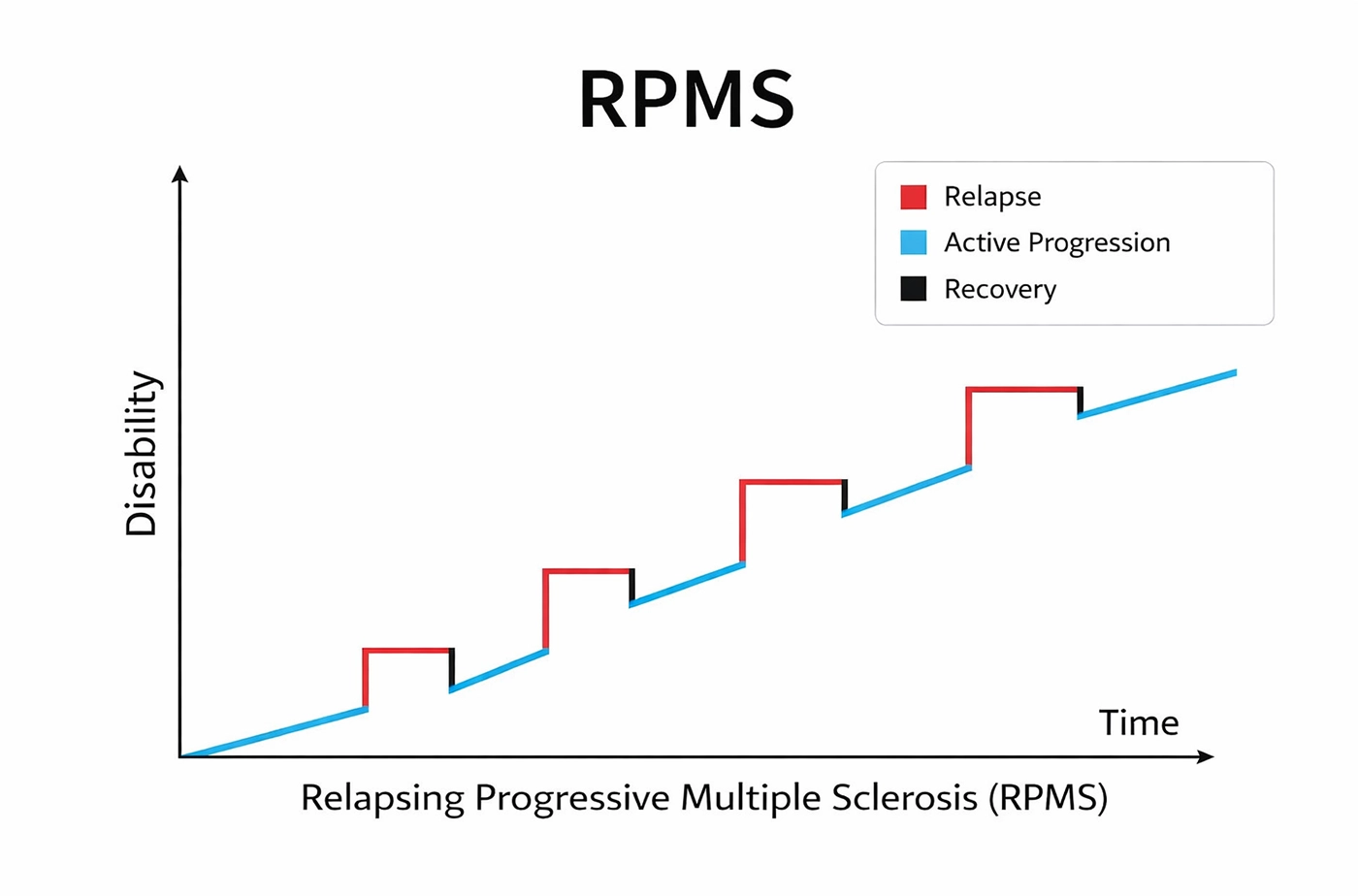
PRMS was historically defined as a form of MS in which symptoms steadily worsened from the beginning, with occasional relapses occurring along the way. It was considered rare, affecting about 5 percent of individuals with MS.
Today, PRMS is no longer classified as a separate type. These cases are generally described as progressive MS with activityor active primary progressive MS (PPMS), although the term may still appear in older references to the traditional four-type framework.versation.
Understanding Progressive-Relapsing MS
PRMS was described as a pattern in which gradual worsening occurs from the beginning, with occasional relapses occurring along the way. It combines steady progression with intermittent inflammatory activity.
Key features include:
- Progression from onset: Ongoing, gradual worsening of symptoms starting early in the disease course, without an initial relapsing-remitting phase.
- Superimposed relapses: Periodic flare-ups in which symptoms temporarily worsen, similar to relapses seen in RRMS.
- Rare occurrence: Historically estimated to account for approximately 5 percent of MS cases.
- Clinical overlap: May initially resemble primary progressive MS (PPMS) until a relapse occurs.
- Updated terminology: Now typically classified under “progressive MS with activity” rather than as a separate type.
The gradual progression reflects cumulative nerve damage over time, while relapses are associated with episodes of inflammatory activity.
How PRMS Affects Daily Life?
Living with PRMS involves managing both gradual progression and intermittent relapses. The combination can affect daily routines in several ways:
- Gradual baseline changes: Walking and balance may slowly become more difficult. Stamina can decrease, and everyday tasks may require more time and effort.
- Relapse-related changes: Periodic flare-ups may temporarily worsen mobility, vision, strength, or sensation. Recovery can be partial or complete, though some residual symptoms may remain.
- Persistent fatigue: Ongoing fatigue may feel disproportionate to activity levels and can limit endurance throughout the day.
- Muscle and sensory symptoms: Weakness, stiffness, pain, numbness, tingling, or burning sensations can make routine activities such as household tasks or computer work more challenging.
- Cognitive and mood changes: Slowed thinking, difficulty concentrating, or mood fluctuations can affect work, communication, and planning.
- Bladder or bowel symptoms: Urgency or frequency may require adjustments to schedules and daily routines.
- Unpredictability: While progression may be gradual, relapses can occur unexpectedly, requiring flexibility in planning.
Supporting daily function
Helpful strategies may include:
- Pacing activities to conserve energy
- Using mobility supports when appropriate
- Participating in physical or occupational therapy
- Keeping a simple symptom log to track changes over time
- Discussing with a neurologist whether the disease appears “active” (relapses or MRI changes), as this can influence treatment decisions
Ongoing communication with the care team is essential to adapt management strategies as needs change.
How Doctors Diagnose Different Types of Multiple Sclerosis?
There is no single test that determines the type of multiple sclerosis (MS). Diagnosis is based on a combination of clinical history, neurological examination, imaging studies, laboratory testing, and observation over time. Your neurologist evaluates what symptoms occurred, when they developed, how they changed, and whether they followed a relapsing or progressive pattern.
The McDonald criteria are the internationally accepted diagnostic guidelines used to confirm MS. These criteria combine clinical findings, MRI evidence, and sometimes cerebrospinal fluid results to determine whether MS is present and whether the disease course is relapsing or progressive. They also help identify whether the disease is currently considered “active.”
Tests Used to Identify MS Types
Healthcare providers use several tools to confirm a diagnosis of multiple sclerosis (MS) and determine the disease pattern. Each test provides different information that helps guide classification and treatment decisions.
- Magnetic Resonance Imaging or MRI (brain and spinal cord) This test is the primary imaging tool used in MS and is often considered the most valuable diagnostic test.
- Detects lesions in areas commonly affected by MS
- Demonstrates dissemination in space and time, meaning lesions occur in different locations and at different points in time.
- Gadolinium contrast dye can highlight areas of active inflammation.
- Follow-up MRIs help identify new or enlarging lesions and signs of atrophy.
- Helps distinguish between relapsing disease (new inflammatory lesions) and progressive disease (gradual clinical worsening with fewer new lesions).
- Lumbar Puncture (Cerebrospinal Fluid or CSF) This test collects cerebrospinal fluid (CSF), the clear fluid that surrounds the brain and spinal cord.
- Tests for oligoclonal bands, which are immune-related proteins frequently found in people with MS.
- Provides supportive evidence when MRI findings are unclear or atypical.
- Can be especially helpful in progressive presentations or complex diagnostic situations.
- Evoked Potentials (especially visual) They are tests that measure how quickly electrical signals travel along nerve pathways.
- Visual evoked potentials are most commonly used in MS evaluation.
- Slowed signal transmission can indicate prior or “silent” nerve damage, even if noticeable symptoms were not present.
- Useful when MRI findings do not fully explain clinical symptoms.
- Neurological Exam and Clinical History A detailed neurological exam and review of your symptom timeline are essential components of diagnosis.
- Assesses strength, coordination, sensation, vision, reflexes, and balance.
- Evaluates whether symptoms occurred as distinct relapses or gradual progression.
- Helps distinguish between relapsing-remitting MS and primary progressive MS.
- Assists in identifying a potential transition to secondary progressive MS over time.
- Blood Tests Blood testing helps rule out other conditions that may mimic MS.
- Screens for vitamin deficiencies, infections, and other autoimmune or inflammatory disorders.
- Ensures that the diagnosis is accurate and supported by appropriate evidence.
Disease Classification and Descriptors
After MS is confirmed using the McDonald criteria, clinicians classify the disease course as:
- Relapsing, or
- Progressive
Additional descriptors are often added:
- Active or not active (based on relapses or MRI activity)
- With progression or without progression
For a diagnosis of primary progressive MS (PPMS), there must generally be at least 12 months of steady clinical progression, supported by MRI and/or CSF findings.
Why Correct Classification Matters?
- Treatment Choices
- Many disease-modifying therapies are most effective for relapsing forms of MS, where the goal is to reduce relapses and new MRI activity.
- In progressive MS, treatment decisions often depend on whether the disease is considered “active.”
- Care plans may place greater emphasis on slowing progression, rehabilitation, and symptom management.
- Timing of Treatment
- Early and accurate classification allows appropriate therapy to begin sooner.
- Prompt treatment may help reduce long-term disability accumulation.
- Setting Realistic Expectations
- Understanding whether symptoms are driven by relapses, steady progression, or both helps guide goal setting.
- Monitoring can then focus on the most relevant indicators, such as new attacks or gradual changes in walking and function.
- Monitoring Strategies
- Relapsing forms of MS may require closer MRI surveillance to track new inflammatory activity.
- Progressive forms may rely more heavily on clinical assessments, including walking tests, hand function, endurance, and daily functional impact.
- Access to Research and Coverage
- Clinical trials often target specific MS types and activity levels.
- Insurance approval for certain therapies may depend on accurate disease classification.
- Clear Communication
- A shared understanding between patients, neurologists, and the broader care team supports coordinated decision-making and reduces confusion in treatment planning.
Can the Type of Multiple Sclerosis Change Over Time?
Yes. MS types are not permanent. They reflect how the disease is behaving over time, and that pattern can evolve.
A common shift is from relapsing-remitting MS (RRMS) to secondary progressive MS (SPMS), often after 10 to 20 years.
In earlier studies (before modern treatments):
- About 20 to 40 percent transitioned within 10 years.
- Around 50 to 60 percent transitioned by 20 years.
With current disease-modifying therapies:
- Fewer people transition.
- When they do, it tends to happen later.
Regular follow-up allows clinicians to reassess the pattern and adjust classification and treatment as needed.
Why MS Types May Evolve?
Multiple sclerosis can change over time. In the earlier phase of the disease, inflammatory relapses are often the most visible feature. Later, more gradual and less obvious processes may contribute to steady progression.
- Early vs. Later Phase
- In the early stages, inflammation is the primary driver of symptoms, often presenting as relapses.
- In later stages, ongoing low-level damage and gradual nerve loss may lead to steady worsening, even without clear attacks.
- Factors Associated With Earlier Progression
- Older age at disease onset
- Greater disability early in the disease course
- A higher number of early relapses
- Spinal cord involvement
- More extensive or specific patterns of lesions on MRI
- The Role of Neurological Reserve
The brain and spinal cord have a certain capacity to compensate for damage, often referred to as neurological reserve. Over time, silent or accumulated damage may reduce this reserve. As it declines, symptoms are more likely to present as gradual progression rather than distinct relapses.
Importance of Ongoing Monitoring
- Why Regular Follow-Up Matters
- The transition from a relapsing pattern to a progressive pattern is often gradual.
- Changes may only become clear over time, making regular follow-up important for early recognition.
- Consistent monitoring allows treatment plans to be adjusted proactively rather than reactively.
- What Clinicians Monitor
- MRI:
- New or enlarging lesions, which may indicate active inflammation.
- Changes in brain or spinal cord volume over time, which can reflect disease progression.
- Overall lesion patterns that may be associated with future disability risk.
- Clinical Assessment:
- Subtle changes in walking speed or balance.
- Hand coordination and dexterity.
- Fatigue levels and endurance.
- Cognitive function, including processing speed and attention.
- Impact on daily activities and overall function.
- How Classification Guides Care
- Descriptors such as “active” or “not active” help determine whether inflammatory activity is ongoing.
- Identifying progression helps guide long-term treatment planning.
- Decisions may include adjusting medications, changing therapeutic strategies, or placing greater emphasis on rehabilitation and symptom management.
- Practical Steps for Patients
- Keep a simple log of symptoms and energy levels.
- Report gradual changes, not just major relapses.
- Attend regular MRI appointments and follow-up visits to ensure timely adjustments to your care plan.

Managing Symptoms Across Different Types of MS
Managing multiple sclerosis typically involves a combination of approaches rather than a single treatment strategy. Care plans often include therapies that modify the underlying disease process, treatments for relapses, symptom-specific management, and ongoing rehabilitation and lifestyle adjustments.
The approach is individualized and may vary depending on whether the disease course is relapsing or progressive, as well as whether it is currently considered active. Treatment decisions are tailored to reduce disease activity, preserve function, manage symptoms, and support overall quality of life.
Treatment Approaches for Each MS Type
There is no one-size-fits-all treatment plan for multiple sclerosis. Management is individualized and may include disease-modifying therapies, relapse management, symptom-directed treatments, rehabilitation, and supportive care. The approach depends on whether the disease course is relapsing, progressive, or currently active.
- For Everyone: Core Components of Care
- Relapse Management
- High-dose corticosteroids may be used to shorten the duration of significant relapses.
- In severe cases that do not respond to steroids, plasma exchange may be considered.
- Symptom Management
Treatment may address symptoms such as:
- Fatigue
- Nerve-related pain or discomfort
- Spasticity
- Bladder or bowel dysfunction
- Mood changes
- Sleep disturbances
- Cognitive concerns
- Rehabilitation
- Physical therapy to support strength, balance, and mobility
- Occupational therapy to improve energy conservation and optimize home or workplace function
- Speech or cognitive therapy when communication or processing changes are present
- Relapsing-Remitting MS (RRMS) and Active Relapsing Disease (including active SPMS or cases with relapses)
Disease-modifying therapies (DMTs) are central to management. These may include:
- Injectable therapies such as interferons or glatiramer acetate
- Oral medications such as fumarates, teriflunomide, or sphingosine-1-phosphate (S1P) receptor modulators
- Infusion therapies such as ocrelizumab or natalizumab
The goal is to reduce relapses and MRI activity. If new relapses or lesions occur despite treatment, therapy may be adjusted or escalated.
- Secondary Progressive MS (SPMS)
Active SPMS(with relapses or MRI activity):
- Medications such as siponimod may be considered.
- In selected cases, therapies such as ocrelizumab may be appropriate based on individual factors.
- Non-active SPMS:
- Emphasis is placed on rehabilitation, mobility support, and symptom management to preserve function and independence.
- Primary Progressive MS (PPMS)
- Early Active PPMS:
- Ocrelizumab is currently approved for treatment and may help slow disease progression in appropriate candidates.
- Later or Non-active PPMS:
- Focus shifts toward rehabilitation, spasticity management, pain and bladder care, and the use of assistive devices to maintain daily function.
- Progressive MS With Relapses (Previously PRMS)
- Management may combine therapies used for relapsing disease with strategies commonly applied in progressive MS.
- Treatment decisions depend on whether inflammatory activity is present.
- Ongoing Reassessment
Treatment plans are regularly reviewed and adjusted as needed. Routine follow-up visits and MRI monitoring allow healthcare providers to refine medication choices, adjust rehabilitation strategies, and align care goals with changes in disease activity or progression.
Lifestyle Adjustments That May Help
Daily habits can support medical treatment and help maintain function. The goal is consistency over perfection. Strategies should be individualized based on energy levels, symptoms, and overall health.
- Stay Active
- Combine aerobic activity, strength training, and balance work as tolerated.
- A physical therapist can tailor a safe, effective program.
- Manage Energy
- Break tasks into smaller steps and schedule rest periods.
- Use cooling strategies if heat worsens symptoms.
- Start Rehabilitation Early
- Physical therapy supports mobility and balance.
- Occupational therapy helps optimize daily tasks and home or work setups.
- Speech or cognitive therapy can address communication or thinking concerns.
- Support Sleep and Mental Health
- Maintain a regular sleep routine.
- Consider stress-management approaches such as mindfulness or counseling.
- Emotional health is an important part of MS care.
- Maintain General Health
- Avoid smoking.
- Keep up with routine medical care.
- Manage other health conditions.
- Aim for balanced nutrition and proper hydration.
- Use Supportive Tools
- Mobility aids or home modifications can enhance safety and independence.
- Early use of appropriate supports often helps maintain function.
- Work With Your Care Team
- Stay connected with your neurologist and rehabilitation providers.
- Track symptoms between visits to identify gradual changes.
Note:These are general recommendations. Your care plan should be individualized based on your MS type, disease activity, and personal goals.
Final Thoughts
MS is defined by patterns of disease activity, not by personal identity. Your classification reflects how the condition is behaving at a given time and may evolve. Terms such as relapsing versus progressive, and active versus not active, help guide treatment decisions, monitoring strategies, and insurance documentation.
Key takeaways:
- Relapsing disease: Early use of disease-modifying therapies aims to reduce relapses and limit new MRI activity.
- Progressive disease: If inflammatory activity is present, certain medications may be appropriate. Regardless of activity level, rehabilitation, symptom management, and structured energy conservation remain essential.
- Track changes: Keep a record of symptoms, energy fluctuations, and gradual changes to share during medical visits.
- Ask clear questions: Discuss whether your MS is currently active and whether there are signs of progression, as this influences treatment planning.
- Prioritize consistency: Regular movement, planned rest, adequate sleep, and stress management support overall well-being.
- Use supportive tools when needed: Mobility aids, braces, cooling strategies, and home modifications can help maintain independence.
- Engage your care team: Collaboration with your neurologist, MS nurse, rehabilitation specialists, mental health providers, and support networks strengthens comprehensive care.
MS management is dynamic. As the disease pattern changes, treatment strategies may also be adjusted. Open communication with your care team ensures that your management plan continues to align with your current needs and goals.
Frequently Asked Questions
Which type of multiple sclerosis is most common?
Relapsing-remitting MS (RRMS) is the most common type at diagnosis. Approximately 80 to 90 percent of individuals are initially diagnosed with this form.
Can multiple sclerosis change from one type to another?
Yes. Over time, RRMS may transition to secondary progressive MS (SPMS). Earlier studies suggested this often occurred within 20 years. With modern disease-modifying therapies, fewer individuals make this transition, and it typically happens later.
Do all types of MS have the same symptoms?
Many symptoms overlap across all types of MS, including fatigue, numbness or tingling, weakness, balance difficulties, vision changes, bladder or bowel dysfunction, and cognitive changes. The primary difference lies in the pattern. Relapsing forms involve episodes of worsening followed by recovery, while progressive forms involve gradual, steady change.
Is one type of MS more severe than others?
Progressive forms of MS, such as SPMS and PPMS, are generally associated with more consistent accumulation of disability over time. However, disease course and severity vary significantly between individuals.
How are types of multiple sclerosis diagnosed?
Diagnosis begins with confirming MS through clinical history, neurological examination, MRI findings, and sometimes cerebrospinal fluid analysis or evoked potential testing. The disease course is then classified based on symptom patterns over time, such as relapsing versus progressive, and whether the disease is currently active or progressing. Classification may be updated as the condition evolves.