Introduction
How does endometriosis affect fertility is one of the most pressing questions women with this condition bring to their doctors. The answers are more layered than most people expect. For some women, endometriosis creates significant barriers to conception.
For others, the impact is far more subtle. Understanding what is actually happening inside the body gives you a clearer picture and, more importantly, a more grounded sense of what your options look like.
Key Takeaways
- Endometriosis affects fertility through inflammation, scar tissue, and reduced egg quality, but it does not make pregnancy impossible for most women.
- Diagnosis is often delayed by 7–10 years because symptoms are frequently dismissed as normal period pain.
- The stage of endometriosis does not reliably predict the severity of symptoms or the degree of fertility impact.
- Early specialist input, a thorough fertility assessment, and an integrative care approach can meaningfully improve outcomes for women with endometriosis.
What Exactly Is Endometriosis?
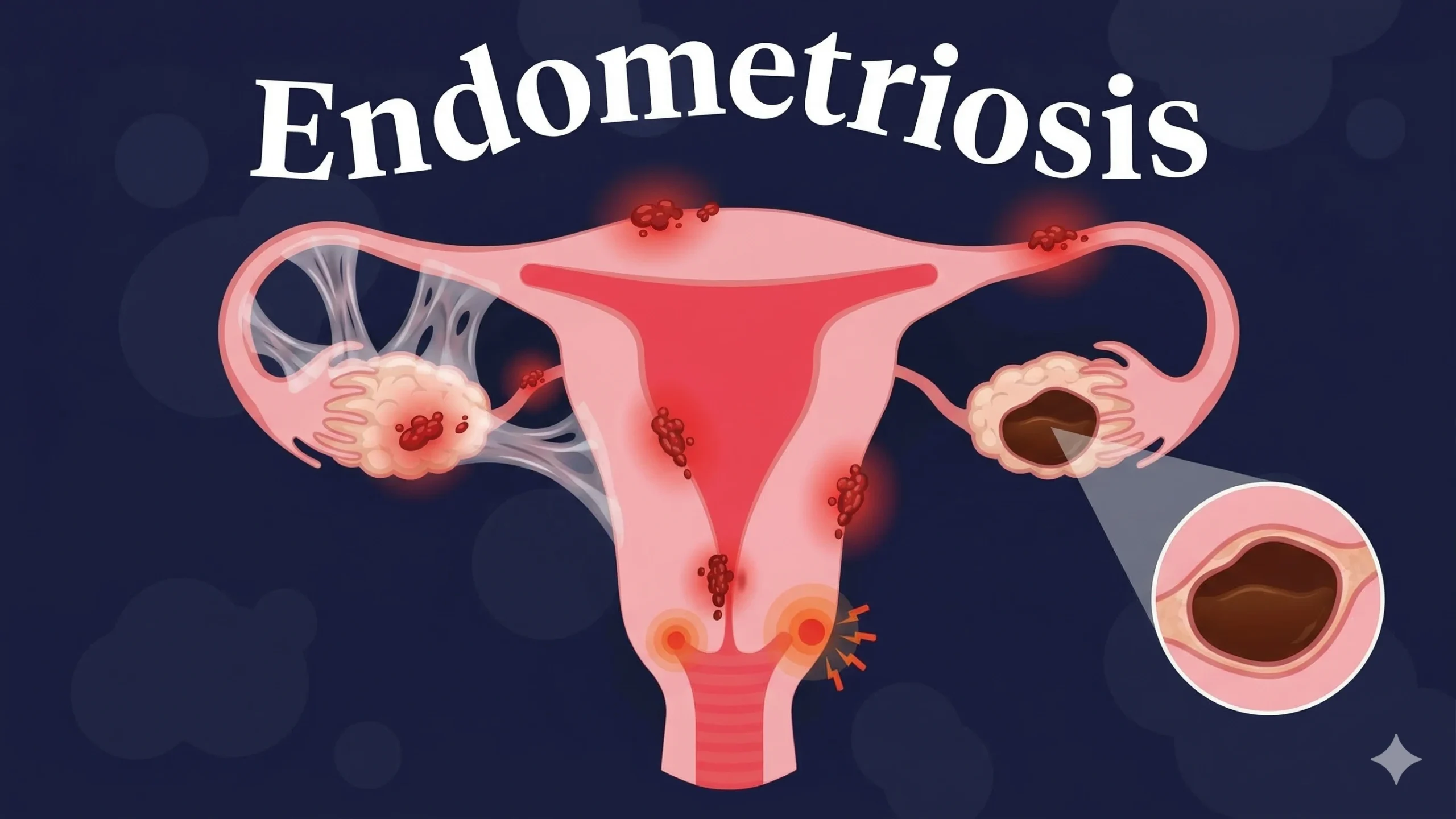
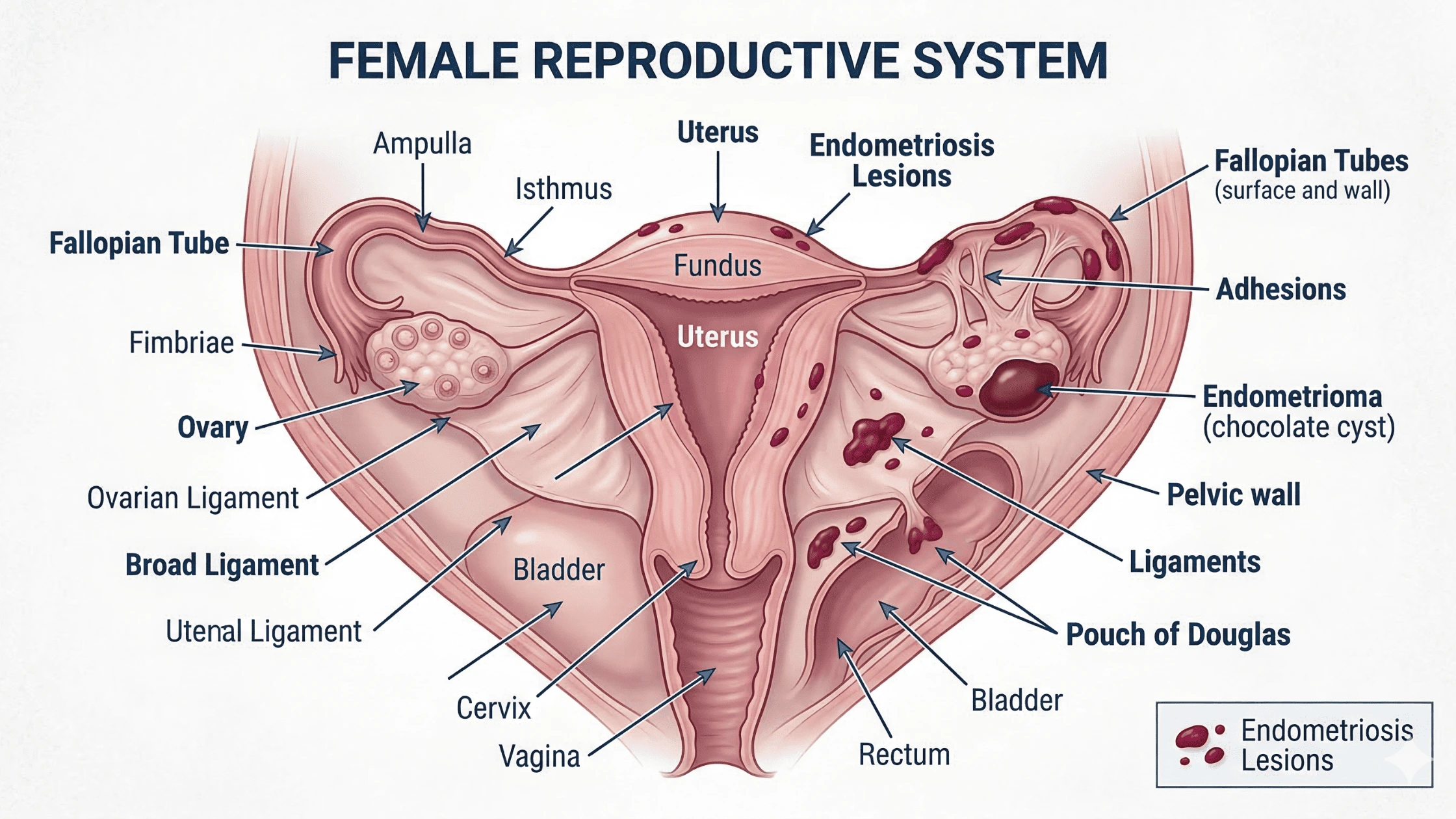
Endometriosis is a chronic condition where tissue similar to the lining of the uterus grows outside of it. This tissue can appear on the ovaries, fallopian tubes, bowel, bladder, and other pelvic structures.
Unlike the uterine lining, it has nowhere to go during a menstrual cycle, causing inflammation, scarring, and sometimes cysts known as endometriomas. It affects roughly 1 in 10 women of reproductive age, though many researchers believe this number is underreported because diagnosis is so often delayed.
How Does Endometriosis Develop in the Body?
There is no single agreed-upon cause, but current understanding points to several key mechanisms:
- Menstrual blood flows backward through the fallopian tubes into the pelvic cavity, carrying endometrial-like cells with it.
- These cells attach to nearby structures and begin growing, responding to hormonal signals just like uterine lining tissue.
- Each month, this misplaced tissue attempts to shed but cannot exit the body.
- The result is ongoing inflammation, tissue damage, and the gradual buildup of scar tissue over time.
Why It Often Goes Undiagnosed for Years?
The average time between symptom onset and a confirmed diagnosis is still estimated at seven to ten years in many countries. Pelvic pain is frequently dismissed as a difficult period. Symptoms overlap with conditions like IBS and pelvic inflammatory disease.
The only definitive way to confirm endometriosis is through surgery, which is rarely the first step. This long diagnostic gap matters for fertility because the longer disease goes unrecognised, the more time it has to cause structural damage to reproductive organs.

Common Signs and Symptoms of Endometriosis
Symptoms vary considerably between individuals. Some women with advanced endometriosis have minimal pain, while others with mild disease experience debilitating symptoms. Knowing what to look for helps with earlier conversations with a doctor.
Pain Symptoms Many Women Experience
Pain is the most common feature of endometriosis and can take several forms depending on where the tissue has grown and how far the disease has progressed:
- Cyclical pelvic pain that intensifies before and during a period
- Deep, persistent ache that can be present outside of menstruation
- Pain during or after sex, often described as deep and internal
- Bowel or bladder pain that worsens around the time of a period
Period Changes That May Signal Endometriosis
Changes to menstrual bleeding are frequently associated with endometriosis and are worth raising with a doctor, particularly when they have worsened over time or do not respond to standard pain relief:
- Heavy periods that involve flooding or passing large clots
- Needing to change protection more frequently than expected
- Spotting between periods
- Periods that have progressively worsened in terms of pain or flow
Other Health Signs That Are Often Overlooked
Beyond pain and bleeding, several other symptoms are commonly attributed to unrelated conditions, which is part of why endometriosis remains underdiagnosed for so long:
- Significant bloating that worsens cyclically, often called "endo belly"
- Persistent fatigue linked to systemic inflammation
- Constipation, diarrhoea, or painful bowel movements during a period
- Ongoing tiredness that does not resolve with rest
Endometriosis vs Adenomyosis: What Is the Difference?
These two conditions are separate but related, and they are sometimes confused with one another. Understanding the distinction matters for both diagnosis and fertility planning.
Where Each Condition Develops in the Body?
Endometriosis involves tissue growing outside the uterus, attaching to structures throughout the pelvis. Adenomyosis involves endometrial-like tissue growing into the muscular wall of the uterus itself, often causing the uterus to become enlarged and tender. Both conditions can occur together, and research suggests this combination is more common than previously thought.
Why Can the Symptoms Feel Similar?
Both conditions are driven by hormonal sensitivity. Because both respond to oestrogen, both worsen during reproductive years and tend to ease after menopause. Shared symptoms like heavy periods, pelvic pain, and painful intercourse mean one condition is often missed while the other is being treated. For fertility planning, adenomyosis raises its own concerns around implantation and uterine receptivity, and both need to be considered when they are present together.

How Doctors Diagnose Endometriosis?
Diagnosis requires a thorough and layered approach. Many women move through several practitioners before getting a confirmed answer, and understanding the process can help you advocate more effectively for yourself.
Early Conversations with Your GP or Specialist
A detailed symptom history is the starting point. A doctor will ask about the timing, character, and severity of pain, changes in menstrual bleeding, bowel and bladder symptoms, and the impact on daily life. Family history is also relevant since endometriosis tends to run in families. A pelvic examination may reveal tenderness or nodules, but a normal examination does not rule out the condition.
Tests and Scans Used to Detect Endometriosis
Several investigations help build a picture of the extent of disease, and they are often used in combination rather than in isolation:
- Transvaginal ultrasound is usually the first imaging step and can identify endometriomas and deeply infiltrating disease in skilled hands.
- MRI provides more detailed information for complex presentations, particularly when bowel or bladder involvement is suspected.
- Blood tests are used to rule out other conditions, though there is currently no reliable blood marker specific to endometriosis.
- A thorough physical examination remains part of the process, even when imaging results are available.
When Laparoscopy May Be Recommended?
Laparoscopy is the gold standard for diagnosing endometriosis. It involves a small surgical procedure under general anaesthetic where a camera is inserted to directly view the pelvic organs and take tissue samples for confirmation. Laparoscopy is typically recommended when symptoms are significant, imaging is inconclusive, or fertility difficulties may be related to endometriosis. Treatment can often be performed at the same time as diagnosis.
The Stages of Endometriosis and What They Mean
The American Society for Reproductive Medicine uses a staging system from Stage I (minimal) to Stage IV (severe), scored based on what is observed during laparoscopy.
Mild to Severe Endometriosis Explained
Endometriosis is classified across four stages, scored based on what is observed during laparoscopy. Stage I and II describe small implants with little or no scarring. Stage III involves more implants, possible small endometriomas, and some adhesions. Stage IV is the most severe, with large cysts, extensive adhesions, and significant distortion of pelvic anatomy.
Does Stage Always Match the Level of Symptoms?
Not reliably. Some women with Stage IV disease report manageable symptoms, while those with Stage I disease can be significantly affected. Fertility difficulties can occur across all stages. This is why stage alone should not drive treatment decisions. The location of disease, individual symptoms, and fertility goals all matter considerably.
Why Does Endometriosis Happen?
The exact cause of endometriosis is still an active area of research. Most evidence points to a combination of factors rather than one single cause.
The Role of Retrograde Menstruation
Most women experience some degree of retrograde menstrual flow, yet only a subset develop endometriosis. This suggests that immune dysfunction plays a meaningful role, allowing misplaced cells to survive and grow rather than being cleared by the body’s normal immune response.
How Genetics May Increase the Risk?
Having a first-degree relative with endometriosis significantly raises a woman’s own risk. Studies suggest the heritability of endometriosis is moderate to high, with specific gene variants identified in large research studies, though no single gene causes the condition on its own.
Environmental and Hormonal Factors
Endometriosis is oestrogen-dependent. Higher lifetime oestrogen exposure, influenced by factors like early onset of periods or shorter cycle length, appears to increase risk. Research into environmental oestrogens found in certain plastics and pesticides is ongoing, though evidence in humans remains preliminary.
How Endometrial Cells May Spread Through the Body?
Beyond retrograde flow, endometrial-like cells may reach distant sites through the lymphatic system or bloodstream, which helps explain rare cases found in the lungs or diaphragm. Another proposed mechanism, coelomic metaplasia, suggests certain pelvic cells may transform into endometrial-like tissue under specific hormonal conditions.
How Endometriosis Can Affect Fertility
Understanding how endometriosis affects fertility requires looking at several biological mechanisms at once. The impact is rarely simple or linear, and it differs considerably between individuals.
Inflammation and Its Impact on Reproductive Health
Endometriosis creates a state of chronic pelvic inflammation that directly affects the environment surrounding the reproductive organs. Research has found elevated inflammatory cytokines and activated immune cells in the peritoneal fluid of women with endometriosis. This altered environment can impair sperm function, reduce egg quality, and affect the uterine lining’s receptivity to an embryo, all without structural changes visible during surgery.
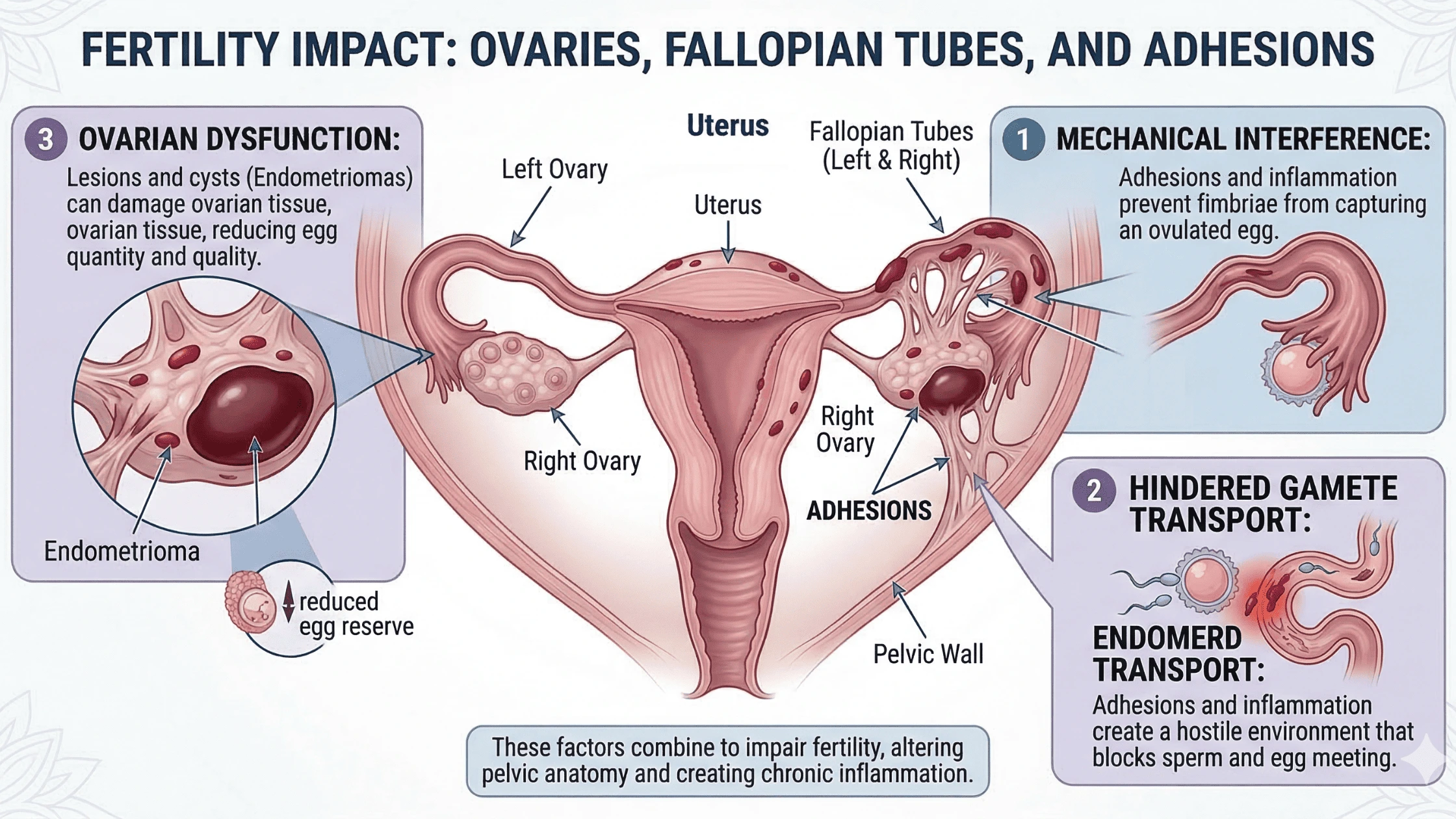
How Scar Tissue and Adhesions Affect the Reproductive Organs?
Repeated cycles of inflammation produce scar tissue that can bind pelvic organs together and distort their normal anatomy. The effects on reproductive function can be significant:
- Fallopian tubes may become blocked or tethered, preventing eggs from travelling normally toward the uterus
- Ovaries may become fixed to the pelvic wall or bowel, limiting follicle development
- Endometriomas can compress or replace healthy ovarian tissue, reducing egg reserve
- Adhesions can restrict movement between organs, affecting both function and surgical access
Changes in Egg Quality and Ovulation ?
Oxidative stress within endometriomas creates a hostile environment for surrounding follicles. Studies have found lower fertilisation rates and poorer embryo development in women with endometriomas compared to those without. Ovulation itself can also be affected. A phenomenon called luteinised unruptured follicle syndrome means a follicle develops but fails to release an egg properly. Hormonal imbalances may also impair the luteal phase, reducing progesterone support after ovulation.
Why Some Women with Endometriosis Still Conceive Naturally?
Many women with endometriosis conceive naturally, some without even knowing they have the condition. The impact on fertility is probabilistic, not absolute. Women with Stage I or II disease, particularly those who are younger and have no tubal involvement, often have fertility outcomes similar to the general population. Even with more severe disease, natural conception remains possible, though monthly chances may be lower than average.
Can You Get Pregnant with Endometriosis?
Yes. Many women with endometriosis do get pregnant, and the majority who want to conceive will either conceive naturally or with appropriate support. The question is less about whether pregnancy is possible and more about understanding the individual picture and what may need attention.
Natural Pregnancy Possibilities
Studies suggest that roughly 70% of women with mild to moderate endometriosis will conceive without medical intervention within two years of trying. This shifts with disease severity, age, and ovarian reserve. Subfertility and infertility are different things.
Subfertility means conception takes longer than expected, not that it cannot happen. Many women with endometriosis fall into the subfertility category and may simply need more time, closer monitoring, or targeted support.
Factors That Influence Fertility Outcomes
Several factors shape the fertility picture for women with endometriosis, and understanding them helps with planning and decision-making:
- Age, since ovarian reserve naturally declines over time and endometriosis can accelerate this process
- The presence and size of endometriomas and whether they are affecting ovarian reserve
- Whether the fallopian tubes are blocked or structurally compromised
- Ovarian reserve markers like AMH and antral follicle count, which guide timing and treatment decisions
- Prior surgeries, since repeated operations on the ovaries can reduce the egg supply over time
Treatments That Help Manage Endometriosis Symptoms
Treatment is personalised and depends on whether pregnancy is a current or future goal, alongside the severity of symptoms and disease extent.
Pain Management Options
Several approaches are used to manage endometriosis-related pain, and the right combination depends on pain severity, location, and individual response:
- NSAIDs like ibuprofen reduce prostaglandins that drive inflammation and cramping
- Prescription pain medications for women whose pain is not managed by over-the-counter options
- Heat therapy for cyclical pain relief without pharmacological side effects
- Pelvic floor physiotherapy for women with associated pelvic floor dysfunction
- Referral to a pain specialist for complex or chronic pain presentations
Hormonal Treatment Approaches
Hormonal therapies suppress ovulation and reduce oestrogen levels, which limits endometriosis growth. The main options include:
- Combined oral contraceptive pill to regulate and suppress the cycle
- Progestogen-only treatments including tablets and the Mirena IUD
- GnRH agonists or antagonists that create a temporary menopause-like hormonal state
These approaches are not suitable while actively trying to conceive, as they suppress the cycle entirely
Lifestyle Support Including Acupuncture
Complementary approaches are used alongside medical treatment by many women and can meaningfully improve day-to-day symptom management:
- Acupuncture has a well-established safety profile and some women find it helpful for pain and stress reduction
- Pelvic-focused yoga and breathwork can support nervous system regulation
- Stress management practices are relevant given the bidirectional relationship between chronic stress and inflammation
These options work best as additions to, not replacements for, specialist medical care
Vitamins and Nutritional Support
Certain nutrients may support symptom management and are increasingly discussed in endometriosis care:
- Vitamin D for its anti-inflammatory and immune-regulating properties, with some studies noting lower levels in women with endometriosis
- Omega-3 fatty acids from fish oil for their documented anti-inflammatory effects
- Magnesium to support pain relief and sleep quality
- Supplementation is best guided by a healthcare provider based on individual testing and needs
Lifestyle, Diet, and Fertility with Endometriosis
Day-to-day choices can support how the body manages inflammation and reproductive health, even if they cannot resolve endometriosis on their own.
Foods That May Help Reduce Inflammation
An anti-inflammatory dietary pattern is broadly recommended for women with endometriosis. Several specific food groups are worth prioritising:
- Fatty fish, walnuts, and flaxseeds for omega-3 fatty acids
- Colourful vegetables and fruits for antioxidant support
- Whole grains and legumes for fibre and gut health
- Fermented foods to support the microbiome and immune regulation
- Reducing processed foods, refined sugars, and high amounts of red meat, which are associated with higher oestrogen levels and greater inflammation markers
Lifestyle Habits That Support Reproductive Health
Beyond diet, several habits contribute meaningfully to reproductive and hormonal health:
- Regular moderate exercise like walking, swimming, or yoga to reduce inflammation and support hormonal balance
- Consistent, restorative sleep, since sleep quality directly affects immune function and hormonal regulation
- Reducing exposure to endocrine-disrupting chemicals where practical, such as choosing BPA-free containers and lower-toxin personal care products
- Building consistent stress management practices, since chronic stress amplifies inflammatory responses
Challenges Linked to Endometriosis
Beyond fertility, endometriosis carries a range of additional challenges that deserve honest discussion.
Understanding the Risk of Miscarriage
Some studies suggest a modestly elevated risk of early pregnancy loss in women with more severe endometriosis, potentially related to inflammation affecting implantation, altered uterine receptivity, or luteal phase insufficiency. Where adenomyosis is also present, this may contribute additional risk. An elevated statistical risk in a population does not mean an individual will miscarry. Many women with endometriosis carry pregnancies to full term without complications.
Is Endometriosis Linked to Ectopic Pregnancy?
There is evidence that endometriosis, particularly when it involves the fallopian tubes, increases the risk of ectopic pregnancy. Tubal damage and abnormal tubal motility can disrupt the normal movement of an embryo toward the uterus. Women with known tubal involvement should discuss this risk with their doctor and be supported with early pregnancy monitoring.
The Emotional and Mental Impact of Fertility Struggles
The psychological weight of endometriosis is significant and often underacknowledged. Several emotional challenges are common among women managing the condition alongside fertility concerns:
- Anxiety and depression related to chronic pain and uncertain fertility outcomes
- Grief over delayed diagnosis or lost reproductive time
- Isolation from feeling misunderstood by those who have not experienced a chronic pelvic condition
- Relationship strain from the ongoing nature of symptoms and treatment cycles
- Burnout from repeated appointments, procedures, and waiting periods
Seeking psychological support is a practical and important part of managing a chronic condition. Many fertility clinics offer counselling services, and peer support groups provide connection that clinical settings cannot always replicate.
When to Seek Professional Help for Endometriosis and Fertility?
Knowing when to push for specialist input can meaningfully affect outcomes. Delays in care have a real impact when fertility is a concern, particularly as ovarian reserve changes over time.
Signs That It May Be Time to See a Fertility Specialist
Timing matters, and several circumstances call for earlier action than standard guidelines suggest:
- Trying to conceive for 12 months without success if under 35, or 6 months if over 35
- A known endometriosis diagnosis, particularly with endometriomas or prior pelvic surgery
- Significant period pain, pain during sex, or bowel symptoms that suggest undiagnosed or undertreated endometriosis
- Declining ovarian reserve markers identified during routine testing
- Any fertility concern that has not yet been thoroughly investigated by a specialist
Finding the Right Support and Care in Australia
Women with endometriosis can be referred by their GP to a gynaecologist, reproductive endocrinologist, or a specialised endometriosis clinic. The Endometriosis Australia network and RANZCOG both provide guidance on specialist care.
Multidisciplinary care that brings together surgical, fertility, pain management, physiotherapy, and dietitian expertise tends to produce better outcomes than a single-specialist approach for complex cases. If you are looking for practitioners who take an integrative and evidence-informed approach to fertility support, Branchout Wellness is a resource worth exploring.
Final Thoughts
Endometriosis does not automatically mean infertility, but it does mean that understanding your body and getting thorough care matters more than it might for someone without the condition. Research has grown considerably over recent decades, and more is known now about inflammation, egg quality, surgical timing, and ovarian reserve than ever before. If you have been living with endometriosis and wondering what it means for your fertility, the most valuable step is getting a complete picture of where you stand and working with specialists who understand the full scope of the condition.
Frequently Asked Questions
At what age does endometriosis usually start?
Endometriosis can begin as early as the first menstrual cycle, though it is most commonly diagnosed in women in their 20s and 30s. Symptoms often start in adolescence and are regularly attributed to normal period pain for years before proper investigation begins.
Can endometriosis stop you from ovulating?
It does not typically prevent ovulation entirely, but it can impair it. Hormonal disruptions can affect follicle development, and a phenomenon called luteinised unruptured follicle syndrome means a follicle matures but fails to release an egg as expected. These disruptions are not always visible on standard testing.